



Masks Don't Work: Persuading The Persuadable Part 1
Can I change someone's mind about masks for covid?

I recently had what I’d call a Unicorn Exchange on Twitter: an opportunity to persuade someone acting in good faith, that masks simply don’t work for covid. Coastal Strength, with whom I’ve had only good interactions (about strength training), commented on a tweet of mine that he thinks masks work and were an important tool in fighting covid for certain times and places.

I saw a unique opportunity. Someone who is acting in good faith, rather than pure tribalism. Is my case strong enough to change his mind? I replied as follows:
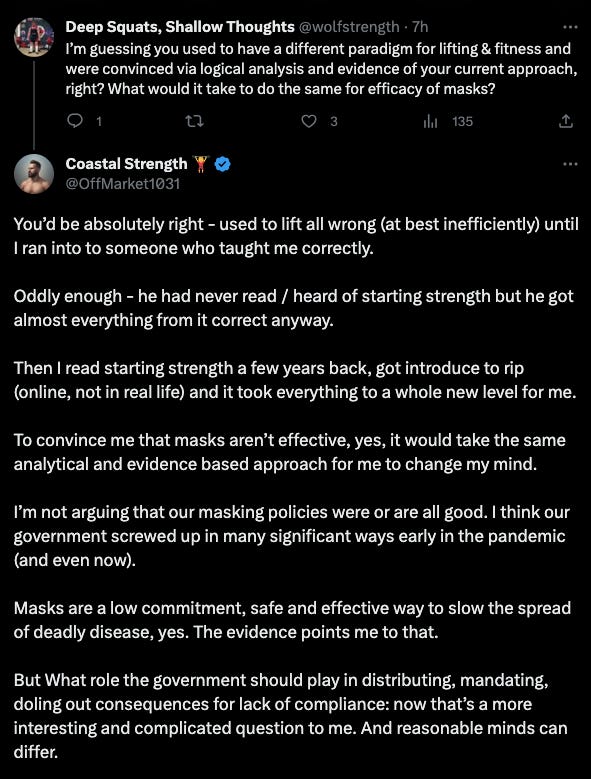
After another few exchanges, in which he sent me a link to his evidence, we agreed on the following terms:
IF I can present enough evidence that masks don’t stop a major primary mechanism by which covid spreads, AND good real world data shows they don’t work, he’d be open to re-evaluating.
Let’s stipulate for the sake of simplicity that when we say masks work/don’t work, we’re using shorthand, not absolute 100% nor 0%, but generally: Does widespread community masking have a significant and measurably good effect or not?
I’ve been posting about masks for 3 years now, first against the mandates, and then once I’d studied more about them, I posted about their inefficacy and downsides too. Can I persuade someone who is willing to change his mind, that they don’t work (per the definition above)? Will he end up changing my mind? Will both of us stay put? This article is my attempt to persuade him, so it will be free of my usual levels of snark. OK, who are we kidding, it won’t be totally fee of snark, but maybe mostly free, because sometimes I can’t help myself. But I’ll be primarily focused on nonpartisan, fact-based persuasion, using a more conversational style than these pieces usually do, and with receipts galore.
Like most times when someone has been persuaded to change their mind, this one will require some reading, some thinking, and then some more thinking. It’s a topic about which whole books could surely be written, so though this article is long, it couldn’t be otherwise. So buckle up, take it in bite-size chunks if you have to, because I want to do this topic justice and make use of what I’ve learned over the past few years.
Covid Era Demands for Masking
It seems pointless to cover how constantly we were told in 2020-2021 that masking was absolutely crucial, and one of, if not the most important things we could do to stop the spread of covid. Anyone who lived though that time remembers how it was broadcast constantly from elected officials, public health officials, and every corporate press outlet. It wasn’t just a recommendation, but mandates and fines were put into place across most of the country and world, and the public was whipped up into a frenzy to see anyone not complying as nearly guilty of murder.
However, just for completeness, here are some examples. First, examples of people being accosted for not wearing a mask due to the intensity of the propaganda, second, of doctors/media/public health emphasizing how important and effective masks are.
Let’s keep in mind that if people were truly afraid of the virus, they wouldn’t be willing to get so close as to physically accost or arrest people for not wearing a mask. The unscientific and hyperbolic rhetoric of doctors and the media around masks, empowered bullies and low status people to have an excuse to assault and lord it over others, while wearing the false guise of empathy. Many such cases:
A woman in Canada was beaten to death in the hospital for not wearing a mask.
A Ohio woman was tased and arrested for not wearing a mask at a middle school football game.
A woman in Australia choked and pinned down by police for not wearing a mask outside.
10 year old student slapped by her school bus driver for not wearing a mask.
An Asian woman on the NYC subway was attacked by a group for not wearing a mask.
A woman was assaulted at Walmart in Utah for not wearing a mask.
A 17 year old student was physically forced out of school and arrested for not wearing a mask.
A man was assaulted in Kansas City for not wearing a mask in a parking lot.
This doesn’t happen without the government and media going on a 24/7 campaign about how amazingly well masks stop the spread of covid and how crucial it is for EVERYONE to wear one, and how selfish you are if you don’t. In the summer of 2020, a doctor told me being against masks was like someone who purposely passes out rats during an outbreak of the plague.
Now, here’s just a few of the endless examples of how the efficacy and importance of masks was pushed by doctors, media, and public health.
Vanity Fair: If 80% of Americans wore masks, cases would plummet:

Former CDC Director Redfield: masks protect better than a vaccine:
Fauci, in summer 2021 on MSNBC: Wear a mask, any mask, don’t worry about what kind:
Dr. Mike Saag, infectious disease specialist and Associate Dean for Global Health at the University of Alabama med school: cloth masks reduce transmission by up to 90%:
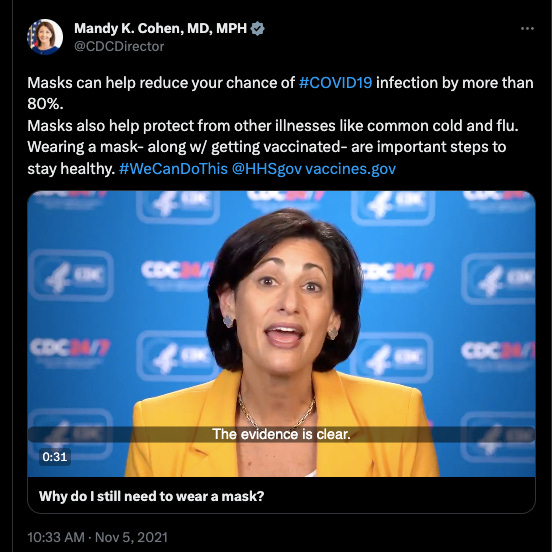
The new CDC director Mandy Cohen, quoting then-CDC director Walensky in late 2021, that masks reduce covid transmission by 80% (what happened to 90%?):
Here’s Fauci’s new replacement as head of NIAID pushing masks over and over again as a crucial measure:
I could fill up a novel with more examples, but we all lived through it and remember, so these will do. Public health, doctors, and the corporate press all hammered us with the message that masks are an essential, effective tool, not just a marginal one, and people attacked others for not wearing one, people refused to see family and friends who wouldn’t wear one. It happened to me, and it happened to some of you, too. This was the direct result of the strong messaging on masks by doctors, the media, and public health. This is what I’m arguing against through the rest of this article below.
Surrogate vs Primary Endpoints
Before we delve into the evidence and analysis itself, we must clarify an important definition and distinction in research: surrogate endpoints vs primary endpoints.
A primary endpoint, in layman’s terms, is the direct actual thing you want to study. Examples in our case here: Does masking reduce covid transmission, does it protect the wearer, does it serve as source control to protect others from an infected wearer? These would all be primary endpoints. In strength training research, a primary endpoint might be an actual increase in weight lifted, or increase in muscle cross-sectional area or circumference. It’s the direct item of interest itself.
A surrogate endpoint, defined by the National Institutes of Health, is a biomarker intended to substitute for a clinical endpoint. A proxy. Note at the link that they say, “although workshop participants agreed that these considerations apply primarily to situations where trials using clinical endpoints are not feasible.” We’ll return to this in the epidemiology and counter-evidence sections in future installments.
An example for masking: “Does masking reduce the number of respiratory droplets that the wearer, or those around the wearer are exposed to?” Not measuring the actual effect on infection or transmission, but droplets - a proxy, a substitute for the thing we actually want to measure. In strength training, examples might be whether a particular exercise protocol results in muscle-protein synthesis, or mTOR activation, instead of measuring actual muscular size or strength increases.
It seems clear that if available, good evidence on a primary endpoint (do masks actually reduce transmission in the real world?) is more persuasive than on a surrogate endpoint (does a mask taped to a mannequin in a lab block droplets?), especially when the connection between the surrogate and the primary is not well established, as we shall soon see is definitely the case in masking.
Before covid, there was an abundance of primary endpoint evidence that masks do not work, so let’s dig into it.
Evidence on Masks in the Pre-Covid Era
A CDC-published Meta-Analysis of the RCTs
Our first stop is this meta-analysis of Randomized Controlled Trials (RCT) on community masking from early 2020, published by the CDC’s own journal, Emerging Infectious Diseases : Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures. It’s important to specify nonhealthcare settings, as that’s the context of this entire discussion and article: masks out in the community, in our day to day lives.
After careful evaluation of the evidence of 14 RCTs up to that point, the authors conclude as follows: Although mechanistic studies support the potential effect of hand hygiene or face masks, evidence from 14 randomized controlled trials of these measures did not support a substantial effect on transmission of laboratory-confirmed influenza. We similarly found limited evidence on the effectiveness of improved hygiene and environmental cleaning. We identified several major knowledge gaps requiring further research, most fundamentally an improved characterization of the modes of person-to-person transmission.
The conclusion was despite some surrogate markers showing potential benefit, the real world evidence to date did not support much use for facemasks in reducing transmission.
But the line at the end there is key, and is echoed again at the end of the entire article:
Further research on transmission modes and alternative interventions to reduce influenza transmission would be valuable in improving pandemic preparedness.
What does this mean? Despite **100+ years of study,** as of Spring 2020, the mechanisms of influenza transmission were still not yet well known enough for us to be confident in the connection between surrogate and primary endpoints. Think about that for a moment as you recall how, beginning in Spring-Summer 2020 when covid was just discovered a few months prior, every public health official and establishment news outlet in the country insisted with absolute certainty that masks were a crucial tool in stopping or slowing the spread of covid.
Are you starting to doubt yet? Not only were masks not found to work for flu - a pathogen thought to be quite similar in presentation and mechanism of spread to covid - but after 100 years of research, we still aren’t 100% sure about all of its mechanisms of spread either. And yet a mere few months after discovery, we were somehow 100% sure that masks would be crucial in stopping covid. If you’re not starting to at least scratch your chin yet, please tell me why.
The WHO 2019 Pandemic Influenza Playbook
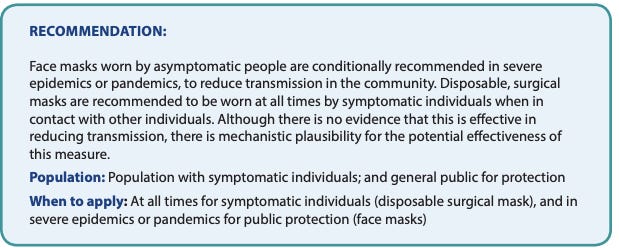
Our second stop is the WHO 2019 Pandemic Influenza Guidelines. A recap of 10 RCTs found mechanistic plausibility, but not enough real world evidence to recommend masks for pandemic influenza:

Now here it gets interesting, because despite the lack of evidence, which they admit, they conditionally recommend it anyway if the pandemic is SEVERE, and handwave a bit about surrogate endpoints. Seems like they’re inserting their opinions here rather than following the evidence, doesn’t it? Regardless, at least they admit there’s no evidence that this is effective, so their recommendation can be viewed as a mere opinion.
One more thing before we move on. The WHO guidelines also mention in this section, that we still have much to learn about how influenza is transmitted (this is back in 2019):

This dovetails with what the Xiao et al CDC paper said 9 months later in 2020. We really don’t fully understand the mechanisms of how flu is spread, and thus our ability to mitigate or control it is still limited. The WHO rated the evidence quality here as moderate; if we take that rating at face value, it’s not “settled science,” but is also not based on only low quality and poor evidence. Not there there ever really is literally such a thing as settled science that can never be challenged, but it speaks the level of certainty in our presumption here, at least according to the WHO. It wasn’t the highest, but there also wasn’t any good evidence at this point to suggest masks did work.
Once again, this leads to the question: How was it possible for anyone to know that masks would work in April 2020? When the CDC began recommending masks and many states and locales enacted mandates, we’d only just discovered covid’s existence a few months prior and still didn’t know how it spread. Do you remember when people were washing their groceries and leaving their mail out for 4 days? THAT’S when masks started being mandated, and almost every state and local govt, and the entire corporate press, jumped on board. We were groping in the dark, and regardless of what was discovered later, it’s impossible to believe that at that point, they knew masks would work so well that it was justified to mandate them. Assumptions about surrogate endpoints while ignoring evidence on primary endpoints doesn’t seem to me like a solid application of the scientific method.
Note as well that they never changed their April 2020 recommendation to mask, to this day. The removal of mask mandates has only been under the justification that we don’t need them anymore, not that masks don’t work as well as initially claimed. The official line of the CDC director, as of February 2023, was that they were so sure masks worked that they didn’t even need to do an RCT on masks during covid. You can watch the whole testimony here, but this is the text of the relevant part:
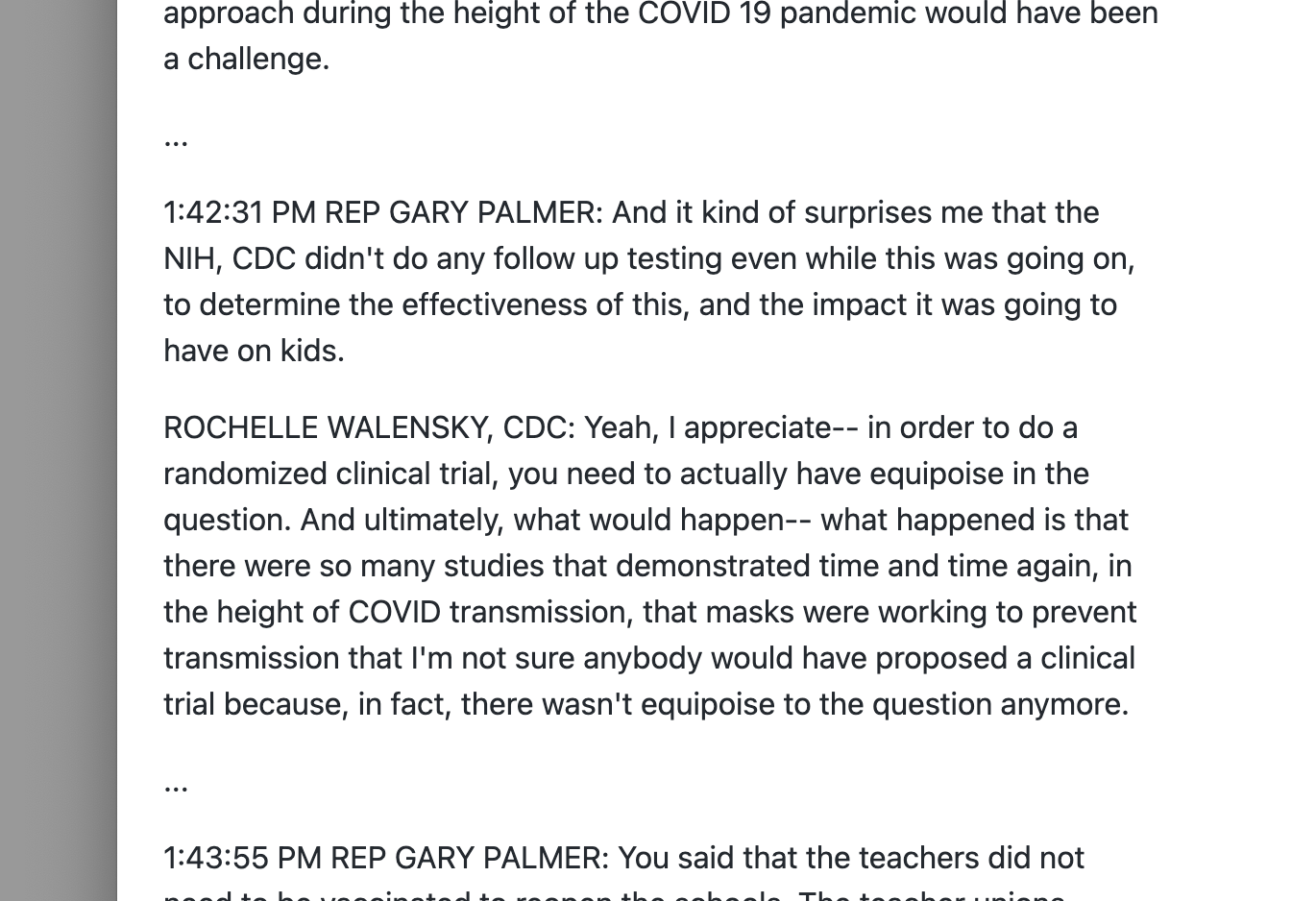
We are already in very sketchy territory indeed. After 100+ years of studying the flu, both the CDC and WHO were willing to admit we don’t understand all of its transmission mechanisms. But a few months into covid, when people were still washing their groceries, we did. Riiiiiiight.

The 2006 Biosecurity Paper by the Epidemiologist who Eradicated Smallpox in Africa
Finally, we have the excellent 2006 paper Disease Mitigation Measures in the Control of Pandemic Influenza, co-authored by epidemiologist D.A. Henderson, who led the smallpox eradication mission in Africa in the 60’s & 70s. This paper is important for its direct contra-indication to everything we did during covid. It concluded against border closures or stopping travel, against lengthy school closures if we do any at all, against lockdowns or quarantines, against masks, and advised to try to continue life as normally as possible:

Wow. What high quality evidence emerged between 2006 and 2020 to completely do a 180 on all of that? Which pandemics was it tested on? I’ll let you ponder that for a moment, while we return to the focus on masks. Here is the mask section:
“There are few data available to support the efficacy of N95 or surgical masks outside a healthcare setting. N95s need to be fit-tested to be efficacious, and are uncomfortable to wear for more than an hour or two.” Since we are only talking about the community: surgical (and a priori, cloth) masks are inherently ineffective, and as for N95s, no one in the community setting is realistically a) fit testing their N95, B) changing into a new one every 2 hours, or C) wearing it with all necessary hygiene, doffing, and donning protocols. No one. Realistically, a lot of people IN health care settings aren’t doing that either. I went to see a dermatologist in Fall 2021, and the whole office was wearing N95s and constantly adjusting and touching them and their faces. The doctor himself did so at least 5 times during the 10 minutes he was with me.
Don’t forget this old favorite from 2020:
Even for trained healthcare workers, an Annals of Internal Medicine observational study found that N95s don’t really protect highly compliant healthcare workers from COVID any more than regular masks, which is to say not at all. A 2019 JAMA-published RCT on N95s for influenza found similar results.
So even when highly trained medical staff wear fit-tested respirators in healthcare settings, the case for them being any better than the ineffective surgical or cloth masks in community settings is far from airtight (rimshot!). We’ll see later that epidemiological data in the community setting supports this for covid well.
Here’s another smattering of evidence against masks from the pre-covid era:
National Academy of Medicine 2018 presentation by Pulitzer Prize journalist Laurie Garrett. She says the only large scale studies that show any mask efficacy at all, are because the mask keeps people far away from each other, not because of any inherent efficacy of the masks themselves. This certainly rules them out in situations like airplanes. Start at the 41:40 mark if not timestamped.
Laurie has ironically become a mask fiend in the covid era, showing just how deeply the response to covid was emotionally and tribally driven.

and still deep into 2023:

Sad!
Our next miscellaneous testimony comes from a 2011 panel hosted by the center for health security. Like the 2006 paper above, the panel (which DA Henderson participated in), was prescient in discussing and being against so much of the stuff we did during covid. Here are two choice segments from Henderson. The first discusses how the government will blunder around doing dumb, ineffective things in order to claim to be doing something:
This should sound very familiar, as Donald Trump still brags to this day about how his early travel restrictions and border closures saved lives (nope), yet his political opponents are even worse, attacking him for not doing enough when obviously what he did was too much - exactly the thing Henderson warned about in 2011! Just goes to show how the Overton Window of political debate on this topic keeps us from debating the truth. I have friends who believe Trump was playing 4D chess here and was doing the best he could get away with under the circumstances, but I am unpersuaded. See what you think:
Looks to me like exactly what Henderson was talking about, and the entire other side that thinks he didn’t shut down enough, didn’t “take covid seriously,” are just even more wrong. But this isn’t a political screed, the point here is Henderson’s prescient point that governments need to be seen as “doing something,” no matter how ineffective or even counter-productive.
The next video from the 2011 conference is on masks specifically, and how they don’t do much.
You can watch the whole panel here, which is full of great nuggets that will upset you if you think the response to covid was scientific rather than political.
Finally, a series of quotes from various sources prior to or very early in the covid era before masking became a tribal marker of virtue:
“The masks worn by millions were useless as designed and could not prevent influenza.” –John Barry, The Great Influenza, 2004.
“The use of fabric materials may provide only minimal levels of respiratory protection to a wearer against virus-size submicron aerosol particles (e.g. droplet nuclei). This is partly because fabric materials show only marginal filtration performance against virus-size particles when sealed around the edges. Face seal leakage will further decrease the respiratory protection offered by fabric materials.” –Rengasamy et al. 2010. Ann Occup Hyg Oct:45(7):789-98.
“In conclusion, our findings suggest that household contacts of persons with symptomatic virus infection are at risk of infection by multiple modes, and that aerosol transmission is important. This is suggestive of the need for further studies into personal preventative measures for the control of influenza; although our observations suggest that hand hygiene and surgical face masks may not provide high levels of protection against influenza virus transmission in these settings.” –Cowling et al. 2013. Nat. Commun. 4:1935. (Randomized controlled trial analysis).
“We know that wearing a mask outside health care facilities offers little, if any, protection from infection…In many cases, the desire for wide spread masking is a reflexive reaction to anxiety over the pandemic.” –Klompas et al. 2020. NEJM. 382;21. (notice how this mirrors Henderson’s 2011 panel comments)
“This study is the first RCT of cloth masks, and the results caution against the use of cloth masks…cloth masks should not be recommended for HCWs, particularly in high-risk situations, and guidelines need to be updated.” MacIntyre et al. 2015. BMJ Open. 5:e006577. (Randomized Controlled Trial)
“Our review of relevant studies indicates that cloth masks will be ineffective at preventing SARS-CoV-2 transmission, whether worn as source control or as PPE.” - Brosseau and Sietsema, 2020. Center for Infectious Disease Reporting and Prevention (CIDRAP). University of Minnesota.
What About Surgeons?
One of the constant rebuttals we heard, and still hear, is: “Oh ya? So doctors (surgeons) have been wearing masks for nothing all these years? I guess you don’t care if your doctor doesn’t wear a mask next time you have surgery! lol you’re so dumb.” Because I’ve encountered this rebuttal countless times, I’m going to share just a small sample of it being used with the typical smug superiority of the midwit. It was downloaded as part of the Covid NPC software patch, and is still making the rounds today. You can find thousands of examples on social media, but here’s a sampling for the record.






I could do this all day.
But you get the picture by now, right? Team Trust The Science first convinced almost everyone that masking was the most sciency thing that ever scienced, and then did nothing to stop the viral idea (pun intended) that surgeons have always masked because of respiratory viruses. They were somehow able to communicate the “Masks work!” message so clearly that by mid-2020, that everyone who Believes That Science Is Real! knew that masks work and whoever didn’t wear one is a Bad Person, but somehow none of them knew that’s not at all why surgeons have historically worn masks.
To respond to this claim, first we’ll do some thinking, then present evidence to validate the theory.
Surgeons wear masks to a) avoid backsplash onto their faces during surgery, and b) to prevent bacteria laden spittle from entering into open wounds, leading to infection. They do NOT, and never have, worn masks to stop the spread of viral respiratory transmitted pathogens. How do you know this? Have you ever had surgery? I’ve had 2 surgeries as an adult, in 2016 and in 2017. In neither case did my surgeon wear a mask at any point except for the surgery itself. When I had my initial meeting and consultation? No mask. When I had my pre-surgery appointment? No mask. When the surgeon came out to see me right before the procedure? No mask. In the OR - mask. At all my follow-up appointments - no mask. Tell me how this makes any sense if the purpose was always to stop the spread of viruses. It doesn’t. It only makes sense if the purpose is specific to the OR during surgery: To protect his face, and to prevent large bacteria-laden spittle from getting into an open body cavity.
Now the question is, does it even work for THAT specific purpose of preventing infections in surgery? While I don’t claim anything definitively, there’s a fair amount of evidence that it doesn’t:
Ritter et al, 1975: “the wearing of a surgical face mask had no effect upon the overall operating room environmental contamination.”
Ha’eri and Wiley, 1980: Put albumin microspheres on the interior of the mask (source control) and then looked for them in the OR and operating field. “Particle contamination of the wound was demonstrated in all experiments.”
Laslett and Sabin, 1989: “No infections were found in any patient, regardless of whether a cap or mask was used.”
Tunevall, 1991: In 1,537 surgeries with masks, post-op infections occurred in 4.7% of cases. In 1,551 surgeries without masks, post-op infections only occurred in 3.5%. Interesting.
Skinner and Sutton, 2001: “The evidence for discontinuing the use of surgical face masks would appear to be stronger than the evidence available to support their continued use.”
Figueiredo et al. 2001: 5 years of peritoneal dialysis without face masks. Peritonitis rates at the unit no different than the ones found in hospitals that used face masks.
Bahli 2009: “No significant difference in the incidence of postoperative wound infection was observed between masks groups and groups operated with no masks.”
Karolinska Institute, 2010: “Our decision to no longer require routine surgical masks for personnel not scrubbed for surgery is a departure from common practice. But the evidence to support this practice does not exist,” wrote Dr. Eva Sellden.
So to sum up:
Surgeons never wore masks to stop viruses, but to protect their own faces and to prevent bacteria from infecting the patient.
It’s not clear if masks even work for the latter purpose, there’s a decent amount of evidence that they don’t, and some places indeed are backing off from some of their longstanding surgery related masking protocols after reviewing the evidence.
Another very interesting point here is that they were able to get approval for these studies - AND surgeons to do the surgeries without them. Yet we were often told during covid, as in this paper: “A hypothetical trial to test the second mode of effect would need masks assigned, or not, to the participants, and to recruit their contacts to compare infection rates between the contacts. Such a trial would be logistically challenging, bordering on infeasible, and potentially unethical.”
This idea was repeated often by many, from comments at the bottom of this paper: “Generating controlled data for mask-wearing is unethical and infeasible,” to being echoed many times by media, as in here in the New York Times: “Researchers would have to require and ensure that people in the mask group wore masks everywhere, while surveilling the other group to ensure no one wore a mask at all. This is not only grossly unethical; it also just isn’t possible...”
Isn’t it strange how, when it came to masks for covid - which were a brand new thing that couldn’t possibly have been studied before since covid didn’t exist or hadn’t been discovered yet - they felt so smug assuming their conclusion in their premise: We KNOW masks work, therefore running a true RCT isn’t ethical because it would deprive people of necessary protection. Interesting. Yet when it came to surgery, where there was a much longer and more well established practice of wearing masks, multiple studies were approved and thousands of procedures performed without masks, and no ethical issue? And these study challenges never seemed to be a deterrent to either conducting RCTs on masks for the flu, nor did it lead to researchers qualifying the evidence based on the studies to be hopelessly weak? Just some more food for thought here.
Regardless, since we now know that surgeons do not and never did wear masks for the purpose of stopping viral pathogen spread, can we stop using that silly line about surgeons now?
Summary of Pre-Covid Masking
I hope I’ve persuaded you by this point that a solid pre-covid consensus, based not on groupthink but on a significant base of evidence, existed against the use of masks in the community setting for respiratory viral protection/transmission. Not that you can’t find a stray bit of evidence for them here or there, but there was a large and solid evidence base against them that was pretty overwhelming in totality. Masks had been studied extensively and found lacking, both as source control and as personal protection, and there was no strong evidence for their efficacy in the community setting. There was no good reason going into covid to think masks worked, or would be an important part of the pandemic strategy, outside of possibly the political reason that Henderson mentioned: the need to be seen as “doing something.” But since so many doctors and scientists knew the truth, surely such a farce couldn’t last long before they called it out, right?
Finally, even if later covid-era studies and real world data somehow showed mask efficacy, the question remains: What changed specifically before April 2020 when they did a 180 and masks were suddenly recommended, then quickly mandated almost everywhere? Fauci’s answer to date has been that asymptomatic spread was a game changer, as he told Gavin Newsom in this 2020 interview.
But the evidence and research to that point told us that masks were ineffective at source control. So why was asymptomatic spread a game changer? (Never mind that asymptomatic spread in 2020 was vastly overstated anyway, as it was found to be less than 1% among house-mates, imagine how much less it was among casual encounters) What actually changed between the entire body of research up to and including the 2006 Henderson Biosecurity paper, the 2011 Henderson panel, the 2019 WHO meta-analysis-based guidelines, and the early 2020 CDC meta-analysis, vs April 2020? Or is it more likely that masks were a political decision all along, which is why they mandated them before possibly knowing they could work, and never changed their tune ever since?
Let all this percolate for a bit, while I finish up Parts 2 and 3 of this series, which will cover the epidemiological/real world data during covid, why the mechanistic surrogate endpoint studies didn’t translate to the real world, responses to some of the most commonly cited studies and evidence FOR masks, and the downsides of masking and why it’s not a harmless intervention.
This is brutal lesson in the power of Brandolini's Law - the effort to refute bullshit exceeds the initial effort to create the bullshit. Here, you have made a massive post, and you are just getting started. Unfortunately I suspect your "unicorn" won't spend the time to even complete part I.
I have studied the mask phenomenon tirelessly the last 3 years [1] and as a lifelong skeptic, I always begin by finding where we can find common ground when debating. Specifically I like to find out where we stand on the following proposals (framed this discussion as I would to your "unicorn", so "you" is not directed at Michael Wolf):
1) What's the lowest "tier" of mask that works?
We both agree that "Fake Masks" [2] do not work. We both agree that Powered Pressurized Personnel Suits aka "Moon Suits" like you see Shi Zengli wearing at a BSL4 lab do work. Somewhere between those extremes is where we disagree. Does a handkerchief work? A Gaitor? A loose fitting cloth mask? Where do they start working? Surgical? Double Surgical?
I propose nothing short of a PPPS Moon Suit works, but to be charitable, I will temporize that a fit tested, single use n95, worn on a freshly shaven face, donned and discarded appropriately, exchanged every 2 hours, could work. I will accept that.
Hopefully you would agree that a cloth mask does not work, which is now the mainstream consensus in science - you need at least a Surgical Mask or N95. (*This is an important concession*, as if the person believes a Cloth Mask works, there is not much hope)
2) Can we agree that in times of crisis, Governments and Figures of Authority will often turn to ineffective solutions with mass appeal just so they are seen as having an answer? Leaders in times of Crisis won't ever say "I don't know" - as their power is derived from knowing. Getting under your desk in the 50's for Nuclear Bomb Alarms was useless but the people in charge wanted to make you feel like they had an answer. "Just Say No" to Drugs was useless in the 80's but it showed the Government was "doing something". George W Bush telling Americans to "go out shopping" after 9/11 was useless. Can we agree that this is a tried-and-true phenomenon?
Can we agree that when political leaders make bad ideas, they are reluctant to admit error? Even obviously stupid bad ideas they will cling to for decades?
I will be proposing that the donning of Face Masks was an example of the Government giving a simple solution to a complex problem to give The People reassurance the Govt was in control. That it would ignite a culture war was unforeseen. In no scenario would the government ever concede "this is a complex problem we won't understand for decades - we don't know"
3) Can we agree what distinguishes science from pseudoscience? I think Carl Sagan framed it best in The Demon-Haunted World:
"Pseudoscience differs from erroneous science. Science thrives on errors, cutting them away one by one. False conclusions are drawn all the time, but they are drawn tentatively. Hypotheses are framed so they are capable of being disproved. A succession of alternative hypotheses is confronted by experiment and observation. Science gropes and staggers toward improved understanding. Proprietary feelings are of course offended when a scientific hypothesis is disproved, but such disproof's are recognized as central to the scientific enterprise.
Pseudoscience is just the opposite. Hypotheses are often framed precisely so they are invulnerable to any experiment that offers a prospect of disproof, so even in principle they cannot be invalidated. Practitioners are defensive and wary. Skeptical scrutiny is opposed. "
Can we agree with Carl Sagan?
I will be making the argument that Mask Science was opposed to skepticism, that like all pseudoscience it cannot predict anything nor produce claims which can be replicated. Most importantly it cannot be falsified. All evidence - all 300 studies showing the wonders of masks - rely on bad science, observational studies, data dredging, and cherry picking. Requests for RCTs are met with opposition and derision, yet the few we have done have found no effect ("but what about Bangladesh" - will address later, though note it found cloth masks ineffective - which were the very masks some 200 other studies used to create this hysteria found 100% effective)
4) Can we agree that science, and in particular medical science, often gets things wrong? And I am not just talking about the ancient past like Galen proposing ingesting mercury, George Washington being killed by bloodletting, or William Farr sticking to Miasma theory a decade longer than the evidence demonstrated - I am talking about our lifetime. Lobotomies. Vioxx. Mammograms under 50. Knee surgery. 100s of medical procedures which were in vogue for years/decades, then were retired. 100s of medications which initially had efficacy, then later found not to be effective.
Perhaps the most relevant recent example is Perdue Pharma convincing tens of millions of physicians that they had developed non addictive heroin using nothing more than sleazy marketing and bullshit science, which would result in a half a million deaths.
Can we agree that often medical science can get things catastrophically wrong? And this is a reminder of the dangers of the "Appeal to Authority"?
I will argue that since it was possible to convince millions of doctors that heroin can be good for (which is an idiotic claim at face value), it is also possible to convince them facemasks can stop viruses (which at least makes intuitive sense before you dive into physics and statistics).
5) Can we agree on some basic facts and physics?
- Covid is airborne
- That a Covid virion is 50 to 140 nanometers (.05 - .14 microns). The smallest visible object to the human eye is 100 microns (think those small mites of dust which are only visible to you when hit with light). This means you could pack up to 11 *billion* Covid virions into the size of that same "almost visible" dust particle.
- The size of the micropore of an n95 is 8 microns. The size of surgical mask micropore is 50 microns. The size of a cloth mask pore is at best 500 microns. To visualize this better, if you scaled a covid virion to the size of a beachball, the size of an n95 micropore would be the size of Epcot center's famous Geodesic Dome. Do the math for surgical and cloth masks
[3][4][5]
- That airflow will follow the path of least resistance. For any mask you wear, the denser the mesh weave, the more the air you breath will push and pull through the sides. Logically the slightest gaps in your mask will be wear air tries to flow through. Even seemingly invisible gaps of a millimeter or two will be where the air will travel (let alone the large gaps you often see by the bridge of your nose). To prove this point, take any of your masks, wear it best you can, and take 5 breaths. Now take that same mask and press it against your mouth forming a tight seal and compare the difference in airflow
- As a reminder, viruses were only discovered in the 1890s after an invisible contaminant passed through *ceramic* chamberland filters [6] which were dubbed "filter passing viruses". Ceramic. Viruses can pass through Ceramic.
Do we agree on these facts?
***
Now that we have established common ground on the above 5 points, I will propose that the facts offer several explanations of why masks have repeatedly failed all and every claim made of their efficacy, These may explain for example, why mask obsessed South Korea has one of the highest excess mortality rates in the world, while all the Nordic countries who weren't too into the masks have the lowest. Why claims such as "Texas is throwing gas on fire" after halting mandates failed to materialize. Why prediction, after prediction failed rendering the hypothesis unfalsifiable.
You will see how we used bad science to support a pseudoscience once again in history.
Great writeup, thanks.